
.gif)
European Journal of Case Reports and Clinical Images
European Journal of Case Reports and Clinical Images
A Case Report | Open Access
Volume 2026 - 2 | Article ID 295 | http://dx.doi.org/10.51521/EJCRCI.2026.e21.110
Academic Editor: John Bose
Corresponding Author: Somarajan Anandan, Department of Neurology, St Joseph
Hospital, Anchal, Kerala, India 691306, Email: drsomarajan@yahoo.co.in
Citation: Somarajan Anandan, Sajeesh
Rajendran, Anandhu Suresh, Joesni Joy (2026). Hot Cross Bun Sign. Euro J Case
Rep Clin Imag. 2026; January, e21, 1-4.
Copyrights: Dr. Somarajan Anandan, 2026 This
article is licensed under the Creative Commons
Attribution-Non-Commercial-4.0-International-License-(CCBY-NC)
(https://europeanjournalofcasereports.com/blogpage/copyright-policy). Usage and
distribution for commercial purposes require written permission.
Keywords: Hot cross bun sign, Multiple sysyem atrophy, Pons, Cruciform
hyperintensity, Verical linear hyperintensity
Case Presentation:
A 67-year-old lady presented with progressive swaying during walking and
dysarthria of five years duration. She also noted bilateral upper limb
incoordination for the last 2 years. She had occasional falls and urge
incontinence. There was no history of any diplopia, dysphagia, weakness, rest
tremor or sensory symptoms. There was no history of syncope but had
constipation. There was no family history of similar illness. On examination
her vitals were normal. Mini Mental Status Examination showed a score of 28 out
of 30. Cranial nerve examination showed gaze evoked nystagmus and scanning
dysarthria. She had hypomimia with mild bilateral appendicular rigidity. She
had normal power in upper and lower limbs with normal deep tendon reflexes.
Plantars were flexor. She had bilateral finger nose incoordination and gait ataxia
with mild postural instability. Autonomic system examination showed a postural
drop of blood pressure of 40/20 mm of Hg. She was treated with
carbidopa-levodopa combination without much improvement. In view of symmetrical
parkinsonism with poor L-dopa response, bilateral cerebellar signs and postural
hypotension, a diagnosis of Multiple system atrophy- cerebellar type (MSA-C)
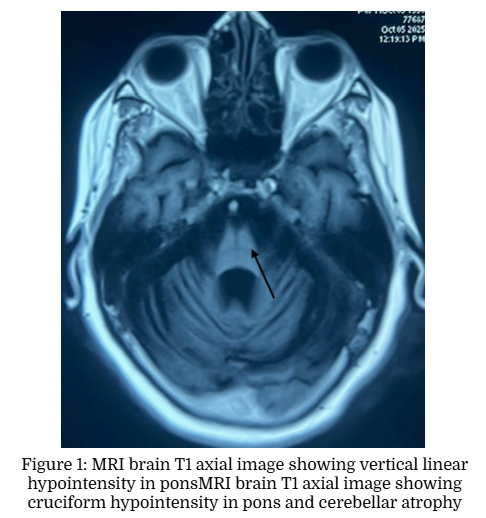
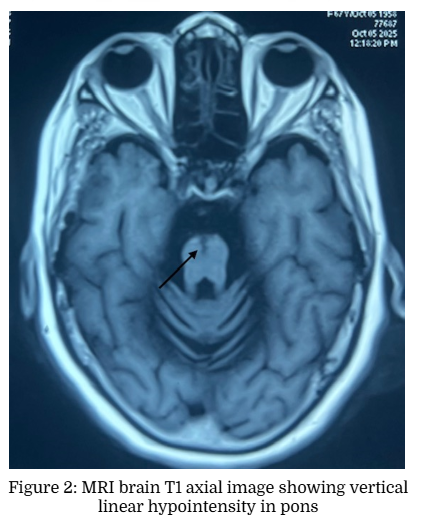
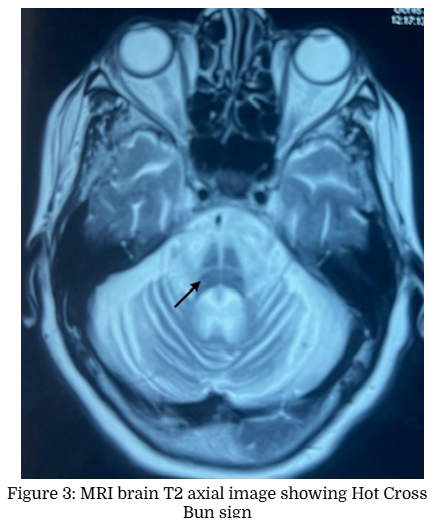
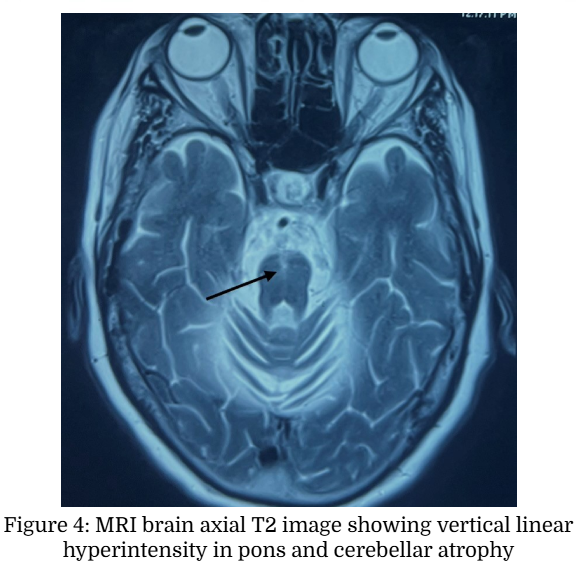
was made and MRI brain was taken. Brain MRI axial T2 weighted images showed Hot
Cross Bun Sign (HCBS) and vertical T2 hyperintensity in Pons. There was
corresponding hypointensity in T1 weighted images Figure (1 to 4).
Multiple system atrophy (MSA) is a neurodegenerative disorder
characterized by parkinsonism, cerebellar ataxia, and autonomic dysfunction.
Early stages of MSA-cerebellar type (MSA-C) is difficult to distinguish from
spinocerebellar ataxias. Various MRI signs like Hot cross bun sign (HCBS),
Putaminal slit sign, middle cerebellar peduncle sign (MCP sign) and inferior
cerebellar peduncle sign (ICP sign) are described in MSA with variable
sensitivity and specificity [1].
The hot cross bun sign (HCBS) is a radiologic finding describing a
cruciform T2 hyperintense signal on axial MRI of the pons, classically
described in MSA. The underlying pathophysiological process is considered to be
atrophy of pontine neurons and transverse pontocerebellar fibers with sparing
pontine tegmentum and corticospinal tracts [2]. It is also reported in patients
with spinocerebellar ataxia (SCA 1, 2, 3, 6, 7, 8, 10, 17, 23, 31, 34, 42),
progressive multifocal leukoencephalopathy, paraneoplastic cerebellar
degeneration from a burned-out testicular tumor, leptomeningeal metastases from
breast cancer, bilateral
middle cerebellar peduncle infarction, cerebrotendinous xanthomatosis, fragile X tremor ataxia syndrome
(FXTAS) and variant Creutzfeldt-Jakob disease [3]. HCBS is graded as Grade 0
(No signal changes), Grade 1 (vertical T2 hyperintensity in ventral pons) and
Grade 2 (cruciform hyperintensity in pons) in axial T2 weighted MRI brain
images [4]. It is reported that the HCBS had a high specificity of 98% to 99%
and a high positive predictive value of 94% to 99% for MSA?, but the
sensitivity was only 45% to 68%. Some of the immune mediated cerebellar ataxia
like anti?Homer 3, anti-Ri and anti Kelch like protein 11 can mimic the MSA?C
phenotype and do not necessarily have a rapid progression [5]. HCBS
also has been described in medulla in adult-onset Alexanders disease [6].
This research received no external funding
Not applicable.
Not applicable.
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Not applicable
The authors declare no conflict of interest.
[1] Lim CY, Seo Y, Sohn B, Seong M, Kim ST, Hong S, Youn J,
Kim EY. The Inferior Cerebellar Peduncle Sign: A Novel Imaging Marker for
Differentiating Multiple System Atrophy Cerebellar Type from Spinocerebellar
Ataxia. AJNR Am J Neuroradiol. 2025 Jun 3;46(6):1223-1230. doi:
10.3174/ajnr.A8623. PMID: 39674591
[2] Gulati, A.; Virmani, V.; Singh, P.; Khandelwal, N. The
hot cross bun sign. Neurology India 57(1):p 104-105, Jan�Feb 2009. | DOI:
10.4103/0028-3886.48790
[3] Prasad S, Rossi M. The Hot Cross Bun Sign: A Journey
Across Etiologies. Mov Disord Clin Pract. 2022 Oct 21;9(8):1018-1020. doi:
10.1002/mdc3.13596.
[4] Sugiyama A, Yokota H, Yamanaka Y, Mukai H, Yamamoto T,
Hirano S, Koide K, Ito S, Kuwabara S. Vertical pons hyperintensity and hot
cross bun sign in cerebellar-type multiple system atrophy and spinocerebellar
ataxia type 3. BMC Neurol. 2020 Apr 27;20(1):157. doi:
10.1186/s12883-020-01738-9. PMID: 32340608; PMCID: PMC7184719.
[5] Liu M, Ren H, Lin N, Tan Y, Fan S, Guan H. The "hot
cross bun sign" in patients with autoimmune cerebellar ataxia: A case report
and literature review. Front Neurol. 2022 Aug 19;13:979203. doi:
10.3389/fneur.2022.979203. PMID: 36062012; PMCID: PMC9437433.
[6] Fang, Xing; Liang, Hui1. Medullary Hot-Cross Bun Sign in
Adult-Onset Alexander Disease. Neurology India 72(1):p 234, Jan�Feb 2024. |
DOI: 10.4103/neurol-india.Neurol-India-D-23-00676.












.png)







.jpg)



.png)